India’s problem - Different drugs, identical brand names
Relevance: GS
- Prelims: Central Drugs Standard Control Organization (CDSCO); Drugs and Cosmetics (Thirteenth Amendment) Rules, 2019.
- Mains: Drug Regulation in India and its associated challenges;
Why in the News?
Recently, an Indian oncologist expressed his shock on social media over the fact that two different drugs, treating entirely different conditions, had identical brand names — ‘Linamac’.
- It is a case of deadly similarity which the medical community has been complaining about for many years, to no avail.
- While the drug bearing the name ‘Linamac 5’ is used to treat multiple myeloma, which is a type of cancer, the other drug bearing the name ‘Linamac’ is a drug used to treat diabetes.
- The consequences of confusion between these medications at the pharmacy can be serious for patients.
What are the various Drug Regulation Challenges in India?
1) An old problem
The use of identical trade names for drugs with different active ingredients is an old problem in India, and the medical community has been complaining about the issue for several decades. For Example:
- The first company uses ‘Medzol’ to sell a drug containing Midazolam which is used as a sedative.
- The second company uses the name ‘Medzole-DSR’ to sell a combination of domperidone and pantoprazole which is used to treat stomach acidity.
- A third company uses the name ‘Medzole 400’ for a formulation containing albendazole that is used in deworming treatment for children.
- A fourth company uses ‘Medzole 200’ for a formulation containing Itraconazole, which is a powerful antifungal drug used to treat diseases such as “black fungus”.
2) Regulatory issue of the Similar Drug Names:
- Language Issue (phonetically and visually similar): The packaging of all drugs in India bears the name and prescription advice in the English language, a language spoken by less than 10% of the population. For example,
- While one company uses the brand ‘Medpol’ to sell paracetamol, a second company uses the brand ‘Medrol’ to sell a corticosteroid and a third company uses ‘Metrozole’ to sell an antibiotic.
- The same company will harvest a successful brand name for one formulation to promote a second formulation. For example, the company that uses the brand name ‘I-Pill’ to sell an emergency contraceptive (ECP) containing Levonorgestrel, uses the brand name ‘i-Pill Daily’ as a daily contraceptive pill containing Levonorgestrel and Ethinylestradiol. An ECP is used after sexual intercourse to prevent fertilization, while a daily contraceptive is used to prevent ovulation and fertilization.
- Indian pharmacies are poorly regulated: Not only do many pharmacies in India routinely dispense drugs without prescriptions, but several also do not comply with the legal requirement to operate only with trained pharmacists who are registered with the Pharmacy Council of India.
- These factors already increase the possibility of errors in dispensing drugs. Add to this deadly combination, identical or similar sounding brand names of drugs, and the possibility of prescription errors increases even further.
3) Data Issues and Political will with in India
- As a country, India has no data on prescription errors. And for the Ministry of Health, the absence of data is the absence of a problem.
- Once the Ministry of Health accepts that there is a problem, it can start the reform process by replicating mechanisms such as those that exist in the United States and Europe.
- Both jurisdictions have specific divisions within their drug regulators to examine the names of drugs on a number of factors to avoid confusion in order to minimize prescription errors.
- There is not an iota of political will within the Drug Regulation Section of the Ministry of Health to undertake similar reforms in India.
What is Judiciary’s Recommendation?
- Cadila Health Care Ltd. vs Cadila Pharmaceuticals Ltd (2001): The SC of India and the Parliamentary Standing Committee on Health and Family Welfare in its 59th report (2012) urged the Ministry of Health to put in place processes to prevent the use of names for drugs that are confusingly similar.
- Further, even the Registrar of Companies and the Office of Registrar of Newspapers for India have systems in place to ensure that no two companies or publications have identical or similar names.
- Regrettably, the recommendations of the Court and Parliament were ignored by the Ministry of Health. But in 2019 it hauled up the Drugs Controller General of India (DCGI) in yet another case of pharmaceutical trademark infringement that landed on her docket.
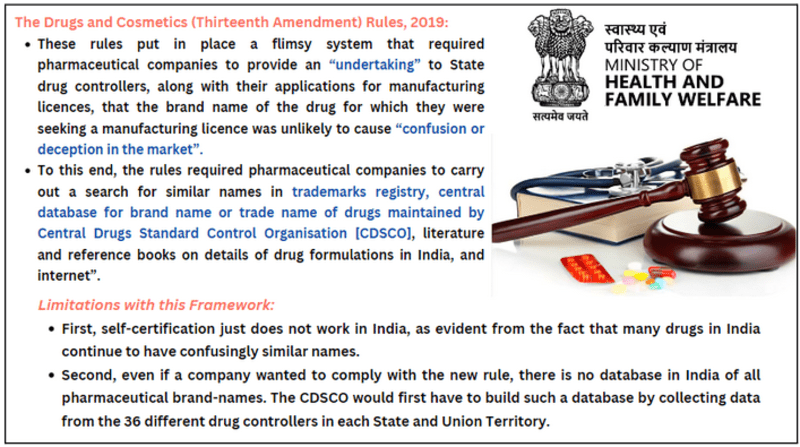
- Under judiciary watch, the Ministry of Health brought in the Drugs and Cosmetics (Thirteenth Amendment) Rules, 2019.
Conclusion: India's drug regulatory system shares some similarities with other countries, it also faces unique challenges and has a more fragmented and outdated regulatory framework. Addressing these challenges and improving the regulatory system is crucial to ensure the safety, quality, and efficacy of drugs in India.
|
BEYOND EDITORIAL Drug Regulatory System in India:
What are the similarities and differences between India’s drug regulatory system and other countries? Similarities:
|
Mains PYQs
Q. What do you understand by Fixed Dose drug Combinations (FDCs)? Discuss their merits and demerits. (UPSC CSE 2013)
Q. Can overuse and free availability of antibiotics without Doctor’s prescription, be contributors to the emergence of drug-resistant diseases in India? What are the available mechanisms for monitoring and control? Critically discuss the various issues involved. (UPSC CSE 2014)
Q. Public health system has limitation in providing universal health coverage. Do you think that private sector can help in bridging the gap? What other viable alternatives do you suggest? (UPSC CSE 2015)